Drugs in sport
Expert reviewers

Essentials
- Almost every professional sport has been affected by claims of doping
- The World Anti-doping Authority (WADA) has banned over 192 performance-enhancing substances and methods
- Many performance-enhancing drugs can pose serious long-term health risks to users
- New performance-enhancing drugs are constantly being developed, as are the methods used to detect them
- Athletes choose to dope for a range of social, emotional and financial reasons
To compete in modern professional sport, to win gold or to hold a trophy high as the flag is raised and the national anthem played is the dream of many. But it will come true for only a few. Only the gifted, only the dedicated, only the best will win.
And maybe a few drug cheats?
Doping
Modern sport is plagued by suspicions that many top athletes resort to drug-taking—doping—to enhance their performance, but this is not a new phenomenon. Its origins can be traced as far back as the ancient Olympics, where competitors would drink ‘magic’ potions or eat special foods to gain an edge over their rivals. The desire to win, motivated by economic incentives such as prizes and large sponsorship deals, or social pressures such as national gold medal expectations, ensures there is a constant market for drugs that will improve performance.
Today, there are as many different Performance Enhancing Drugs (PEDs) as there are sports, and it’s a big job trying to keep track of them all. In 1999, an internationally independent organisation, the World Anti-Doping Authority (WADA), was established. It works to coordinate the fight against doping in sport internationally, and is assisted in this task by organisations around the world such as the Australian Sports Anti-Doping Authority (ASADA), the United States Anti-Doping Agency (USADA) and many others.
Over 192 banned drugs and ‘performance enhancing methods’ (such as blood doping) are registered by WADA, a list which is constantly updated as new drugs emerge. A substance can be considered for inclusion on the World Anti-Doping Code Prohibited List if it meets two of the following three criteria: 1) it is or potentially is performance-enhancing, 2) it is or potentially is harmful to the athlete's health, and 3) it violates the spirit of sport. WADA makes the final determination on whether a substance or method is included on the prohibited list.
Both the creation of these drugs and the methods used to detect them involve sophisticated science, with each side (the makers and the testers) constantly innovating to try and stay ahead of the game.
While cycling, athletics, weightlifting and swimming have been regularly associated with athletes using PEDs, no sport is immune. From archery to yachting and all sports inbetween, athletes have sought out drugs to improve their performance or hasten recovery from injury.
Types of performance enhancing drugs
Among the most popular PEDs are anabolic steroids, human growth hormone, erythropoietin (EPO), beta-blockers, stimulants and diuretics to name just a few. While drugs such as these get a lot of publicity, they are perhaps not well understood. What do they do? What are the health risks in the short or long term? Can the drugs be detected?
Let’s take a look...
Stimulants
Stimulants are drugs that directly affect the central nervous system. They work to speed up parts of the brain and body, increasing the heart rate, blood pressure, metabolism and body temperature of the user. They are used by athletes to reduce tiredness and fatigue, and to increase alertness, competitiveness and aggressiveness.
The most common stimulants detected in anti-doping tests include amphetamines, cocaine, ecstasy and methylphenidate (Ritalin). The actual effects vary according to the drug and to its method of ingestion—drugs that are snorted or injected will produce more immediate results than those that are taken in pill form.
Nicotine and caffeine are also frequently used as stimulants but they are not banned in sports. However, both substances are currently on the WADA Monitoring Program for 2015. WADA is observing them in order to detect potential patterns of misuse in sport.
Health risks
The risks of using stimulants vary for each drug, but in general are high. For example, cocaine use can cause panic attacks and paranoia, lead to the loss of smell and problems swallowing, become addictive and, in rare cases, lead to heartattack. Amphetamines can cause damage to the liver, kidneys and cardiovascular system, and cause hallucinations and violent behaviour, while long term use can change the structures of the brain involved with memory and emotion.
Examples of use
Jamaican sprinter and track star Asafa Powell was caught using the banned stimulant oxilofrine in 2013. A number of Australian athletes have also been sanctioned GLOSSARY sanctioneda threatened penalty for disobeying a law or rule for use of the stimulant methylhexanamine. Read the full ASADA Sanctions list for more information on Australian athletes.
Testing
The presence of stimulants in the body can be tested by a variety of procedures. Urine is the primary means to test for stimulants, although blood (serum) can also be tested and, occasionally saliva. Commonly used tests include chromatography, immunologic assay GLOSSARY immunologic assayan immunoassay may use an antigen to detect for the presence of antibodies, which recognize that antigen, in a solution. , and mass spectrometry GLOSSARY mass spectrometry(MS) is an analytical chemistry technique that helps identify the amount and type of chemicals present in a sample by measuring the mass-to-charge ratio and abundance of gas-phase ions. .

Anabolic steroids
Anabolic steroids are drugs derived from testosterone, a hormone which is produced in the testes of males and, to a much lesser extent, in the ovaries of females. Testosterone is partially responsible for the developmental changes that occur during puberty and adolescence and is also involved in controlling the build-up and breakdown of the main biochemical components of all tissues, including muscle.
There are two types of anabolic androgenic GLOSSARY steroids:
Exogenous steroids are synthetically created versions of the testosterone hormone. These substances cannot be naturally produced by the body.
Endogenous steroids are naturally occurring substances in the human body that are involved with the metabolic pathways of testosterone.
Because testosterone affects muscle growth, raising its levels in the blood can help athletes increase muscle size and strength. Anabolic steroids can be taken in tablet form or injected directly in to the muscle. Some of the most common types of anabolic steroids include:
- stanozolol
- nandrolone
- boldenone
- trenbolone
- androstenedione
- tetrahydrogestrinone (referred to as THG or The Clear).
Athletes who use anabolic steroids claim that as well as increasing muscle mass, they reduce body fat and recovery time after injury. But the androgenic (masculinising) side-effects—such as increased body hair and a deepening of the voice—are not always desirable, particularly in women. To counteract these side-effects, scientists developed steroids that retain their anabolic effects but have a lower androgenic effect.
Examples of use
Androstenedione was used by East German Olympic swimmers and other athletes in the 1970s and 1980s to improve their performances. More recently, American sprinter Marion Jones admitted to using THG (amongst other PEDs) resulting in the disqualification of all her competitive results post-September 2001.
Health risks
Medical experts see significant dangers in the use—and particularly the gross over-use—of anabolic steroids. Some of the effects are minor or only last while the drug is being taken; others are more serious and long-term. For example, anabolic steroids can cause high blood pressure, acne, abnormalities in liver function, alterations in the menstrual cycle in women, decline in sperm production and impotence in men, kidney failure and heart disease. They can also make both men and women more aggressive.
Testing
Testing for anabolic steroids has come a long way since the 1970s, when basic
radioimmunoassay
GLOSSARY
radioimmunoassay(RIA) is a sensitive method for measuring very small amounts of a substance in the blood. Radioactive versions of a substance, or isotopes of the substance, are mixed with antibodies and inserted in a sample of the patient's blood. The same non-radioactive substance in the blood takes the place of the isotope in the antibodies, thus leaving the radioactive substance free.
The amount of free isotope is then measured to see how much of the original substance was in the blood.
techniques were used. Today, anabolic steroids and their by-products can generally be detected quite easily in urine, using mass spectrometry. However, since testosterone occurs naturally and its levels in the body fluctuate daily and can vary from person to person, setting a threshold above which an athlete is deemed to be ‘using’ anabolic steroids remains a subject of debate.
Testosterone and a related compound, epitestosterone, are eliminated from the body in urine. When an athlete takes testosterone or its precursors (supplements which the body can convert into testosterone), the ratio of testosterone to epitestosterone (the T/E ratio) may increase. Prior to WADA, the International Olympic Committee stated that an athlete is guilty of doping if their urine sample shows a T/E ratio above 6.
There are problems with this test. For example, British athlete Diane Mohdahl had a four year competition ban lifted after demonstrating that a high T/E ratio detected in her urine sample could have been caused by bacterial contamination. Another problem is that some athletes have been shown to have a naturally high T/E ratio, so that the threshold of 6 could be set too low. Alternatively, athletes with a naturally very low T/E ratio may not go above 6 even if they are taking additional testosterone.
Today, anti-doping labs use the combined technique of Gas
Chromatography
GLOSSARY
Chromatographya technique for the separation of a mixture by passing it in solution or suspension through a medium in which the components move at different rates.
–Mass Spectrometry (GC-MS) in combination with Gas Chromatography Combustion Isotope Ratio Mass Spectrometry (CG/C/IRMS). This is an analytical method that combines the features of gas-phase chromatography and mass spectrometry to identify different substances within a test sample, effectively detecting differences in the ratio of carbon isotopes in different compounds. This technology can distinguish between testosterone produced naturally by the body (endogenous) and that which is a result of synthetic compounds (exogenous).
Continuing advancements in the detection of steroids (and stimulants) are currently being developed. In the U.S, a research team is working on a detection system that is being touted as a 1000-fold improvement on the commonly used mass spectronomy technique. The new technique, named Paired Ion Electrospray Ionisation (PIESI) makes traces of steroids or amphetamines more visible to current detection equipment by introducing a chemical agent which effectively binds itself to the traces, right down to the parts per trillion.
To develop reliable tests, researchers have to know what they are looking for. This is difficult because the development of new 'designer' steroids is an on-going process. The World Anti-Doping Agency is aware of the problem. In 2003 they were able to develop a test for one of these designer steroids—tetrahydrogestrinone (THG)—when a syringe full of the drug was given to them.

Human growth hormone
Human growth hormone (HGH; also called somatotrophin or somatotrophic hormone) is a naturally-occurring hormone produced in the human body. It promotes physical development—particularly the growth of bone—during adolescence. It stimulates the synthesis of collagen, which is necessary for strengthening cartilage, bones, tendons and ligaments, and also stimulates the liver to produce growth factors.
In adults, HGH increases the number of red blood cells, boosts heart function and makes more energy available by stimulating the breakdown of fat. Other effects attributed to HGH include increase in muscle mass and strength as well as tissue-repairing (recovery). However as HGH is often used in conjunction with other PEDs its direct role in these benefits is unproven. Still, it is quite easy to see why athletes believe it will enhance their performance.
Because HGH is a protein hormone, it is possible to manufacture large amounts of HGH using recombinant DNA technology. Like anabolic steroids, HGH has a legitimate role in medicine—specifically for people with Growth Hormone Deficiency (GHD) or muscle weakness due to HIV—but it is also misused by athletes.
Examples of use
English Rugby player Terry Newton was suspended in 2010 after testing positive for human growth hormone, while Bulgarian sprinter Inna Eftimova was banned from competition in 2012 after a returning a positive HGH test.
In the United States, Major League Baseball continues to negotiate its way through the findings of the BALCO scandal, a PED ring involving HGH and other doping drugs which implicated numerous professional pro-baseball players such as Barry Bonds and Jason Giambi.
Health risks
If you believe all the hype—emanating mainly from drug manufacturers—HGH is a wonder drug that will remove wrinkles, reverse the ageing process, restore vitality and improve sleep. Nevertheless, there are some health risks.
For example, too much HGH before or during puberty can lead to gigantism, which is excessive growth in height and other physical attributes. After puberty, inflated levels of HGH can cause acromegaly, a disease characterised by excessive growth of the head, feet and hands. The lips, nose, tongue, jaw and forehead increase in size and the fingers and toes widen and become spade-like. The organs and digestive system may also increase in size, which may eventually cause heart failure. Acromegaly sufferers often die before the age of 40. Excessive use of HGH in adults may also lead to diabetes; muscle, joint and bone pain; osteoarthritis; cardiac limitations; hypertension; and abnormal heightened symptoms of cardiovascular disease.
Testing
A test for HGH involves two distinct but complimentary approaches: the ‘isoforms approach’ and the ‘markers approach’. A full description of the testing method is available on the WADA website. This dual-approach test has been confirmed as robust and scientifically reliable by the Court of Arbitration for Sport.
Blood doping
Blood doping is the use of various methods and substances to increase a person’s red blood cell mass. Higher levels of red blood cells in the blood result in more oxygen being transported to the muscles, resulting in increased stamina and performance. There are three main types of blood doping:
- erythropoietin (EPO)
- synthetic oxygen carriers
- blood transfusions.
All methods of blood doping are prohibited by the WADA.
Erythropoietin (EPO)
Erythropoietin—more commonly known as EPO—has long been the drug of choice for endurance athletes. Although used in a wide variety of sports, it is most commonly associated with cycling—particularly with the disgraced former champion of the Tour de France—Lance Armstrong.
Produced naturally by the kidneys, EPO is also available as a pharmaceutical. EPO stimulates the production of red blood cells in bone marrow and regulates the concentration of red blood cells and haemoglobin in the blood. This is useful for athletes, since red blood cells shuttle oxygen to the cells, including muscle cells, enabling them to operate more effectively. EPO is a peptide GLOSSARY peptideA molecule consisting of a short chain of amino acids. Longer chains of amino acids are called proteins. hormone and can be produced synthetically using recombinant DNA technology. By injecting EPO, athletes aim to increase their concentration of red blood cells and, consequently, their aerobic capacity. EPO can also work to increase the body’s ability to buffer lactic acid.
Health risks
If EPO levels are too high the body will produce too many red blood cells which can thicken the blood, leading to clotting, heart attack and stroke. In fact, EPO has been implicated in the deaths of numerous athletes, predominantly cyclists. Repeated doses of EPO can also stimulate the development of antibodies directed against EPO, which can result in anaemia. The long-term health risks of sustained EPO use are still unclear.
Examples of use
The 1998 Tour de France hit controversy when the entire Festina team was disqualified after several hundred doses of EPO and other doping products were found in the team car. EPO has continued to be associated with the event ever since, as evidenced by Lance Armstrong’s admissions in 2012 of EPO use throughout his seven tour victories. Other sports associated with EPO use include boxing (Shane Mosley, 2003), 50km walk (Alex Schwazer, 2012) and athletics (Rashid Jacobs, 2008).
Testing
An approved test for EPO was first introduced at the Sydney 2000 Olympic Games. The test used a combination of urine testing, which would identify the presence of EPO (direct test) and blood testing, which would show the residual ‘footprints’ of EPO drug use over time (indirect test).
Methods such as isoelectric focusing, which is the separation of proteins based on their electrical charge, and sodium dodecyl sulfate polyacrylamide gel electrophoresis, which is the separation of proteins based on their size, are used to detect EPO.
Since 2002, EPO tests in the United States were undertaken using only urine, however, in recent years the joint testing methods, such as direct EPO testing in urine and use of indirect blood tests as part of the Athlete Biological Passport (see below), have been used to help identify the use of newly-developed erythropoiesis stimulating agents.
A new testing technique for EPO is also in the pipeline. Researchers are working on a detection method that will look for the effects of EPO in the body’s cellular anatomy as opposed to its presence in urine or blood. In essence the new test will look for genetic expressions which prove that EPO has been used. If the new test proves accurate and viable, it will be almost impossible to use EPO without detection.
Synthetic oxygen carriers
Synthetic oxygen carriers (SOCs) are purified proteins or chemicals that have that ability to carry oxygen. They are still under development and have not been approved for use outside of South Africa and Russia. SOCs were developed for use in crisis situations where blood transfusions are not possible or blood products are not available.
There are several different types of SOCs available. Two of the most common types include haemoglobin based oxygen carriers (HBOCs) and perfluorocarbons (PFCs). Like red blood cells, they work to deliver this oxygen to the muscles, increasing aerobic capacity and endurance. However, they also have some additional benefits. HBOCs are not only great at tissue oxygenation, they can deliver increases in blood serum iron, ferritin and naturally occurring EPO. They can also increase CO₂ production and curb lactic acid production.
PFCs, due to their size, are able to enter the body’s tiny capillaries, providing very efficient local oxygen delivery to greater areas of the body, while the makeup of the drug also allows it to deliver oxygen to peripheral tissues.
SOCs are still under development and testing, and have not yet been proven safe for human use. However, this has not stopped rumours of athletes using them to get an advantage.
Health risks
The health risks associated with using SOCs are similar to those of EPO—increased risk of heart attack, stroke and pulmonary embolism. HBOC’s have not been found safe for human use.
Testing
A complex four-step test was made available for SOCs in 2004. The first step involves the elimination of abundance proteins in blood samples via immunodepletion. Next, capillary electrophoresis (CE) is undertaken, followed by UV/Vis detection. The last step is Time-of-Flight (TOF) or Mass Spectrometer (MS) analysis of the sample.
Blood transfusions
Prior to the introduction of synthetic blood doping drugs like EPO, blood transfusions were common practice among endurance athletes. Even with these drugs available the practice still persists.
Blood transfusion is an effective and relatively simple method of allowing athletes to boost the number of red blood cells in their blood, improving their aerobic capacity and endurance.
Blood transfusions can be classified as autologous, where the athlete receives pre-prepared doses of his/her own blood, or allogenic, where the transfused blood comes from someone else. Athletes who choose to use this method generally begin undergoing blood withdrawals several weeks before a competition, building up a supply of blood between 450 millilitres and 1800 millilitres. The plasma is returned to the body during the withdrawal while the corpuscular elements—basically the red blood cells (RBCs)—are stored. These can then be re-infused in the patient directly before or during a high-endurance event.
The re-infused blood greatly increases the number of red blood cells in the blood, boosting the blood’s ability to bring oxygen to tired muscles.
Examples of use
Blood transfusions were common practice before being banned in 1986. The first known case was Kaarlo Maaninka, who transfused two pints of blood prior to winning medals in the 1980 Olympics. By the 1984 Olympics, one-third of the US cycle team received transfusions, resulting in nine medals.
In 2007 Alexander Vinokourov, a rider in the Tour de France, tested positive after winning the 13th stage of the race. His blood was found to contain two different blood cell populations, which confirmed the use of allogenic transfusions.
Testing
Cheating via blood transfusions was initially difficult to catch, especially if athletes re-infused their own blood. The arrival in 2004 of a test to detect allogenic blood transfusions meant athletes could no longer use the blood of a donor, however, they could still cheat by re-infusing their own. The development of Athlete Biological Passports (see below), has made even this method more detectable, as the passports allow testers to see the indirect markers of blood doping.
Health risks
The risks of using blood transfusions to increase red blood cells is similar to the risks associated with EPO and SOC use: thickened blood leading to clotting, heart attack and stroke. Another risk relates to the process itself. Because transfusions involve several stages—the withdrawal of blood, its storage and re-use—there are many opportunities for something to go wrong. Contamination of the blood or equipment, infection and improper administration of blood products, all of which could easily lead to drastic health problems, even death.

Beta Blockers
Beta Blockers work to block the effects of adrenaline. They work to slow the heart rate, thereby reducing blood pressure, anxiety and muscle tremors, and improving the ability to focus. This makes them particularly useful to athletes performing in sports that require a steady hand such as shooting, archery, darts, snooker, even golf. Beta Blockers are prohibited by several sports (darts, racing) during competition, but others (archery, shooting) prohibit their use at all times.
There are more than 20 types of beta blockers available. They can be taken orally, via injection or (in the treatment of glaucoma) as eye drops. Some common beta blockers include:
- propranolol
- metoprolol
- atenolol
- bisoprolol
- esmolol.
Health risks
When used for a legitimate medical reason, for example to treat a heart condition, high blood pressure anxiety, and under the guidance of a trained professional, beta blockers have a good safety record.
When used without a legitimate health reason, side effects can include reduced circulation through the hands and feet, dizziness, fatigue, dry mouth and drowsiness. More serious (though rare) side-effects can include impotence, asthma attack, memory loss or heart failure.
Examples of use
A high-profile case of Beta Blocker use at the elite level was in 2008, when Olympic shooter Kim Jong-su tested positive for Propranolol and was subsequently stripped of his medals.
Testing
Beta Blockers can be detected in human urine using Gas Chromatography Mass Spectrometry. Many sports will not allow the presence of Beta Blockers at any level, despite an athlete’s claims that it may have been used for a legitimate medical reason.

Diuretics
Diuretics work to promote the production of urine. While putting your hand up for a toilet break may not be deemed professional in modern sport, athletes use diuretics to assist with weight-loss (the loss of water through urination leads to an overall loss of body weight). This is particularly useful in sports where weight is critical such as boxing, rowing or horse-racing. An added benefit of all these toilet breaks is that other drugs present in the system could also more quickly be ‘flushed out’ of the body. The increased urine volume also aids in the dilution of doping agents and their metabolites. All classes of diuretics are considered to be ‘masking agents’ by WADA and are banned both in and out of competition. Diuretics have been banned in sport since 1988.
There are more than 20 diuretics banned by the IOC and WADA. Some examples include:
- hydrochlorothiazide
- desmopressin
- probenecid
- amiloride
- metolazone.
Health risks
When used to treat legitimate medical conditions such as heart failure, high blood pressure, kidney and liver problems and glaucoma, and under the supervision of a trained doctor, diuretic use is quite safe.
However, because diuretics promote frequent urination, when used without medical supervision they can lead to dehydration, dizziness, muscle cramps and constipation. Other side effects include tiredness, fever, skin rash and loss of appetite. More serious effect include disruptions to the normal rhythms of the heart, and electrolyte abnormalities, which can affect kidney function.
Examples of use
Jamaica’s most successful female track athlete, Veronica Campbell-Brown, tested positive for a banned diuretic in 2013. Former Australian cricketer Shane Warne tested positive for a banned diuretic in 2003 and subsequently was suspended from all forms of cricket for 12 months, leading to him missing the 2003 ICC World Cup. Warne claimed to have taken the tablet to ‘get rid of a double chin’ for television appearances.
Testing
Previously, diuretics were detected in biological samples through the use of high-performance liquid chromatography (HPLC) coupled with ultraviolet-diode array detection (UV-DAD). However, this method was not deemed rigorous enough in determining the unequivocal identification of banned substances. For this reason, international anti-doping regulations have required the implementation of mass-spectral methodology to test samples.
A new way of testing
Athlete Biological Passports
Setting the benchmarks above which an athlete is deemed to be a drug cheat is a difficult issue for sporting bodies. High levels of hormones do not always indicate cheating, and low levels do not always guarantee innocence. For example, Finnish cross-country skiing champion Eero Mäntyranta, who won two gold medals in the 1964 Winter Olympics, had a genetic mutation which enabled him to produce unusually high levels of erythropoietin (EPO). How can we set fair benchmarks that catch the cheats but don’t return false positives on athletes operating by the rules?
One solution introduced in 2009 is statistical profiling, which essentially allows testers to create a ‘biological passport’ for each athlete. Athlete Biological Passports (ABPs) are a unique, personalised electronic record of an athlete’s biological values, developed over time from multiple collections of blood samples. The ABP collates data on the levels of different substances in the body, during and after exercise, and uses this to construct a profile, effectively determining natural levels of various substances in the body for each individual. From this information, testers can assess if an athlete suddenly has a large jump in certain hormones or proteins in their blood, when compared against their normal levels. This could indicate that doping has occurred.
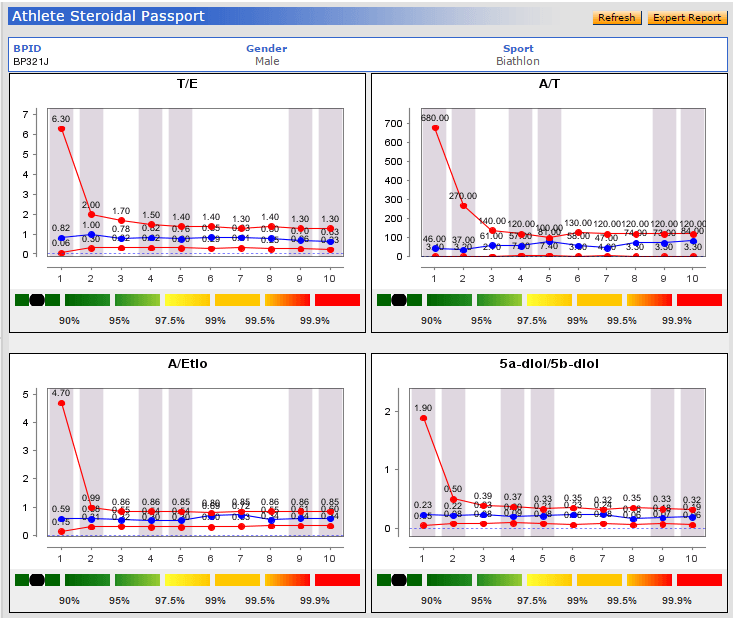
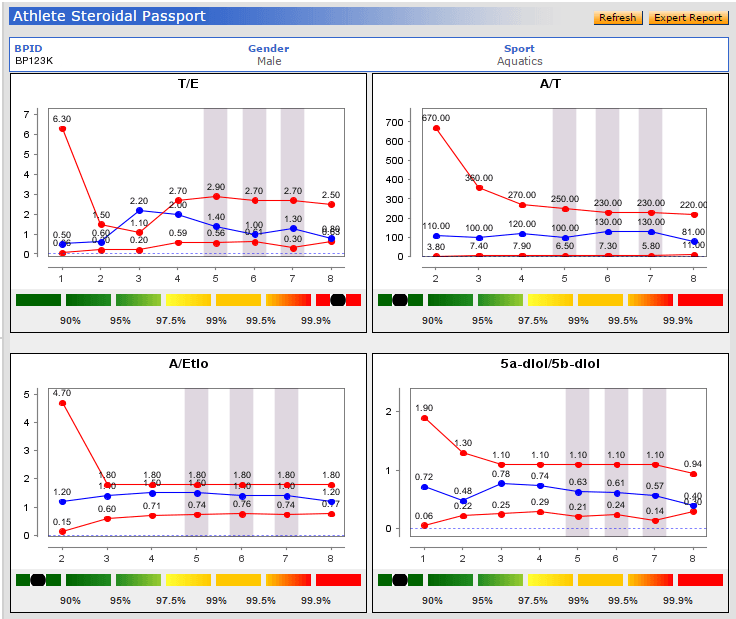
The initial ABPs contained a standardised approach to the profiling of an athlete’s haematological variables (blood module) for the detection of blood doping. Since 2014 ABPs also include a steroidal module, which monitors selected urinary steroid concentrations over time to monitor for potential steroid doping.
The Australian Sports Anti-Doping Authority (ASADA) notes that ‘The ABP differs from traditional detection methods by looking for the effects of blood doping rather than detecting the prohibited substances or methods used. The advantage of this approach is the biological effects of a performance-enhancing agent are commonly present and detectable for a longer period than the agent itself.’ Information gathered from the ABP will be used in conjunction with traditional testing methods, providing officials with additional data with which to determine an athlete’s possible guilt or innocence.
Long term effects of doping
Most athletes dope for short-term gain, but what are the long-term implications of using these drugs? From a health perspective, the verdict is unclear. As listed above, all doping drugs have potential immediate or short-term side-effects and drawbacks, but scientists are still researching the longer-term effects they may have on the body. Some studies have found evidence of early mortality due to cancer or heart attack amongst previous long-term users of PEDs, but these are inconclusive as other factors such as lifestyle, and genetics may also be responsible. Part of the difficulty is in finding athletes who would agree to participate in such a study.
From a performance point of view, scientists from the University of Oslo have released preliminary findings showing that athletes may continue to benefit from having taken banned substances long after the drugs have left their system and their bans have been lifted. The 2013 study, which was undertaken on mice, found that muscles can retain some of the advantages gained through anabolic steroid use for years, possibly even decades after the drugs were taken.
Kristian Gunderson, Professor of Physiology at the University of Oslo said 'If you exercise, or take anabolic steroids, you get more nuclei and you get bigger muscles. If you take away the steroids, you lose the muscle mass, but the nuclei remain inside the muscle fibres. They are like temporarily closed factories, ready to start producing protein again when you start exercising again.'
If proven, their study would require a complete reworking of the current anti-doping system, including length of bans and ability to return to competition. On 1 January 2015, WADA introduced tougher punishments for doping, including upping the bans from two to four years. There are also stronger punishments for coaches, trainers and administrators who are found to have helped athletes dope.

Conclusion
While we would love to believe all athletes compete solely for the love of the game and in the true ‘spirit’ of sport, the truth is that there will always be those who try to find a way —legal or not—to get that competitive edge. More than 2000 years of sports history tells us that when one method is detected, another rises to take its place. As ABBA famously sang ‘The winner takes it all’—at least for a while. Winners may be grinners, but drug cheats can’t win back their reputation.